
Fish Hook Removal

Fish-Hook Removal
Arguably the fishing capital of the United States, Florida has a higher-than-average rate of encounters with fishing hooks. Designed to penetrate fish skin and anchor into flesh while burying deeper with resistance, hooks do exactly that in humans as well. Whether encountered while actively fishing, as an innocent bystander, or spicy Lego in the beach sand; fishing hooks are frequent culprits leading to emergency room visits. There are specific methods to hook removal and considerations for treatment that are important for emergency physicians to be aware of.
Types of hooks and parts
There are three main types of hooks commonly used for fishing. The simplest is a J-hook with a single point and barb parallel to the shank forming J. Circle hooks are similar to J-hooks except for having a rounded shank that curves into an inward-pointing point and barb. The most troublesome of hooks is the treble hook, essentially a trio of J hooks unified by a single shank. The top of a hook that is looped for attachment to the line or leader is called the eye, from there the descending segment to the bend is called the shank. The curved section or bend changes direction from the shank and ends in the point that is most often accompanied by a barb that locks the hook into place once in a fish or person.
A patient presents hooked, now what?
When a patient presents with a fishhook injury there are several important pieces of information to immediately gather and steps to take. Make sure the patient holds the punctured body part still while you examine the wound. Make sure the wound is hemostatic and not life-threatening. Rinse the wound with water or saline. Be sure to isolate the hook by removing any attached bait/line/lures. If the hook has multiple barbs the non-penetrating points should be removed with a multitool or other cutting instruments such as a bolt cutter. Removing the extra hooks and lures will stop further injuries from occurring during removal. It will be important to determine the type of hook before removal attempts. Determining the tetanus vaccination status and any comorbidities that delay healing will be helpful to obtain for post removal management. Depending on the location of the hook, evaluate that the tissue distal for perfusion, sensation, and movement to assess neurovascular integrity. If the eye is included, tape the shank to the face to reduce movement, apply an eye shield and proceed directly to a facility with ophthalmologic services.
Removal techniques
Several standard removal techniques will be highlighted below. Before any removal prep the surrounding skin with chlorhexidine, iodine, or other disinfectants. Be sure to apply local anesthetic locally or as a nerve block when possible. Tools you will potentially need include a pair of pliers or hemostat, 18g needle, string or strong suture material such as silk, bolt cutter or multitool, scalpel, and eye protection
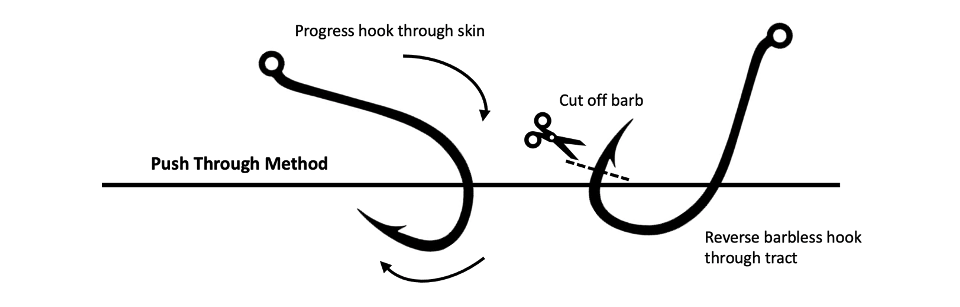
1. Retrograde: The retrograde removal is the gentlest option available and preferred when possible. This technique has the shank pushed down towards the skin to dislodge the barb from the tissue while slowly reversing the point through the skin along the tract of entry to dislodge the hook.

2. Advance and Cut: This method is best for difficult to dislodge hooks through other methods and is hopefully superficial with good anesthetic use. In this method, the hook is advanced until the barb protrudes through the skin at which point the barb is cut off and the hook is backed out easily without the barb impeding tissue
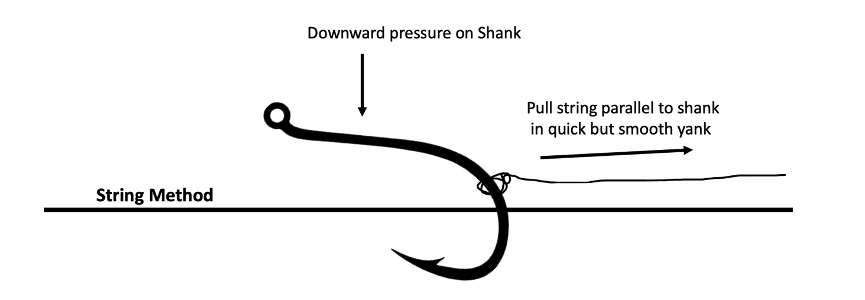
3. String technique: The string technique while tricky to master is very satisfying when successful. In this technique, a string is tied to the bend of the hook and while downward pressure is applied to the shank to dislodge the barb, the string is yanked parallel to the shank in a quick fluid motion.
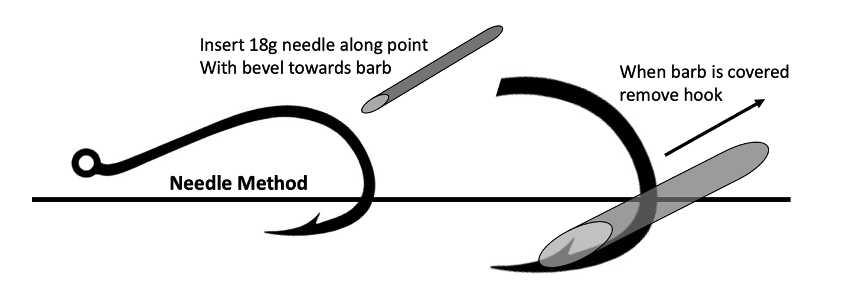
4. Needle Cover: This technique is a bit more difficult but can be useful for awkwardly placed hooks that cannot be advanced or are buried deep. An 18-gauge needle or larger is slid down the hook from the bend towards the point on the barb side of the hook with the bevel facing the barb. If done correctly the needle will cap the barb allowing removal of the hook without the resistance of the barb.
5. Cut Down: If all else fails, a scalpel can be used after adequate local anesthetic and if not in a dangerous location to cut down to the barb creating a tract for removal.

Post Removal care
After the hook is removed, the wound should be irrigated with saline to remove infectious agents the wound should be evaluated for foreign bodies, typically by XR. The wound can have antibiotic ointment applied and may be bandaged with a sterile dressing or band-aid if small enough. There are no indications for oral antibiotics post hook injury, however, they may be considered in patients with immunocompromised status or exceptionally dirty wounds. Most importantly, do not forget the lifesaving TDaP if indicated.
Final thoughts
Fishhook injuries are all too common in Florida and the management should be part of the emergency physician playbook. There are several techniques described in the literature for removal with varying degrees of difficulty and invasiveness that may require some practice to perfect. In most cases, antibiotics are not indicated, although tetanus should be updated when indicated. This skill set should translate well both in your recreational and professional Florida life.

Vincent Costers, MD
USF Emergency Medicine
Vincent Costers is a current PGY-3 Emergency Medicine resident at USF. He completed his medical school training at USF Morsani College of medicine. He is currently working towards completing a Fellowship in the Academy of Wilderness Medicine (FAWM). He also serves as an Academic Chief and Blog Editor for the 2022-2023 academic year.
References:
Auerbach, P. S. (2012). Chapter 24: Hunting and Fishing Injuries. In Wilderness Medicine. essay, Elsevier Mosby.
McMaster, S., Ledrick, D. O. D., & Stausmire, J. (2013). Evaluation of a simulation training program for uncomplicated fishhook removal. Wilderness & Environmental Medicine, 24(3), 292. https://doi.org/10.1016/j.wem.2013.03.013
Prats, M., O’Connell, M., Wellock, A., & Kman, N. E. (2013). Fishhook removal: Case reports and a review of the literature. The Journal of Emergency Medicine, 44(6). https://doi.org/10.1016/j.jemermed.2012.11.058
Photo Credit to Joanna Ennis and her recent incident with a jig to the scalp